

Future of Life Science Pioneered by Biosupercomputing
In order to change from observation-type medical practice focusing on experience to predictiontype medical practice to construct the base of theoretical medicine

Professor, Department of Internal Medicine (Cardiovascular Medicine), Director of the Metabolic
Disease Research Center,
Bio-Research Medical Center, Tokai University Graduate School of Medicine,
and Director, Department of Metabolic System Medicine, Tokai University General Medical Laboratory
Shinya Goto
■For predictive, individual and “prospective” medical practice
━ You often say that the present medical practice is empirical, and lacks logic and predictability.
●Goto (dispensed with the Mr. and Mrs) If I, as a clinician engaged in the
treatment of a large number of cardiovascular diseases, say this, patients
may be shocked, but it is the present state of affairs that when doctors
provide medical care, they do not fully appraise the system of the human
body and disease scientifically, and do not provide medical care based on
definite prediction like controlling an atomic power plant based on physical
understanding, for example. Medical intervention based on an essential
and sophisticated understanding of life phenomena is presently impossible.
It is obvious considering the history of medical progress. Doctors know
empirically what will happen if they do nothing for diseased people. By
making a certain intervention considered to be effective without leaving
patients as they are and observing whether the prognosis (catamnesis) is
good or bad, we are repeatedly evaluating the propriety of intervention.
Medical care has progressed by repeatedly comparing what result will be
obtained if some other intervention is made. Evaluation of experience may
be performed based on the doctor’s own common sense, or based on a
numerical database obtained by summarizing a large number of cases. The
latter method for evaluation of a numerical database based on a certain
standard is also called "Evidence-Based Medicine". However, even Evidence-
Based Medicine which has incorporated scientific methodology is only a
methodology in which cumulative past experience is quantified. Even if
the experience is converted to a numerical database, there is no essential
difference in that past medical practice still decides future directionality
based on “retrospective” experience.
Comparing this to the history of the development of physics, it can be
said that present medical science is still in the age of Galileo. By dropping
a heavy ball and a light ball from a high place at the same time, Galileo
revealed that the time taken for falling is not related to the weight of
object. He revealed the basics of dynamics by an experiment, but he could
not arrive at a future unified principle, that is, the gravity of the earth and
the law of gravitation even control celestial motion. Before long, Newton
extended the law of gravitation by mathematically discussing the motion
of objects discovered by Galileo et al., and constructed the basis of modern
physics. Current medical practice is conducted under circumstances where
the universal life phenomena controlling the human body are not yet
understood. Doctors only describe the patients’ symptoms appearing as
a change in life phenomena and their change according to the presence
or absence of therapeutic intervention, and accumulate experience. Since
we can understand only the “result with or without medical intervention,”
we only evaluate the patient population to determine the propriety of
medical intervention. In order to introduce modern physics and science
like chemistry into the world of medical care, it is necessary to understand
the nature of life phenomena, to clarify the factors defining individual
differences, and then to construct learning like architectural and prospective
“theoretical medicine.” Hence, it is necessary to resolve life phenomena
into factors, and to understand them by fine mathematical expression of
the causal relationship among factors. In the world of medical practice,
a learning system is required which makes “theoretical prediction” and
“individualization” possible. If we cannot have such a system, we will not
be able to take even one step beyond the medical practice evaluated by
accumulation of past experience.
━ Why can we give only empirical medical care?
●Goto In a word, the nature of the problem is that, since the life phenomena constituting the human body are too complex and there are too many factors involved in the onset and progress of disease, we cannot precisely understand the causal relationship among these factors. In order to give the optimum treatment for individual patients, we have to understand the nature of life phenomena, the factors defining individual differences, and the sophisticated causal relationships among them. Genes, a design blueprint of an individual, are different individually, and exposure to environment and life style are different individually. Unless the system, from molecules through cells to the human body, that is, what disease is likely to occur in the human body when a person with a certain gene lives under a certain condition, can be understood architecturally, it is impossible to conduct medical practice and individual medical care with which the future can be predicted scientifically. In order to understand a system where the combination of slight positional differences in an enormous number of genes individually defines optimized therapeutic methods, moreover, it is necessary to handle an enormous amount of integrated time-dependent information such as information about genes, exposure to environment, life style and disease, at the same time. In order to reconstitute clinical medicine as information science, that is, the basis of a precise future-type medical practice in the 21st century, a high-speed supercomputer is absolutely required. We already know information about the design blueprint of the human body defining individual differences called the personal genome. We understand the system in which the design blueprint produces proteins. However, we have not understood the system in which those proteins constitute cells. It is the current state of affairs that although we can understand how the functions of biological molecules will change when a drug consisting of molecules is administered, we cannot understand how the change is constituted in cell response and biological response on the scale of the human body. If we understand the system in which cells and the human body are constituted by physical and chemical interactions of a huge number of molecules, we may be able to understand life phenomena exactly. By so doing, it may be possible to provide scientific treatment in the true sense for the first time.
━ What is the most promising point of the ten quadrillion speed computer “Kei”?
●Goto In order that we can understand life phenomena, I think
that reproduction of life phenomena is important. If all the substances
constituting one cell were arranged positioned spatially, it might be possible,
in principle, to reconstitute the cell. At the present time, there are too many
substances that make up cells, and we have no fundamental technique that
can reconstitute the information. If we establish a technique to measure
information about the arrangement of substances in cells precisely and
enter the information virtually on a high-speed supercomputer, it should be
possible to reproduce virtual cells. We can observe the aspect whereby cells
gather together to constitute tissues and organs at the microscopic level.
Such an approach is the basis of simulation biology, and the ten quadrillion
speed computer is an important tool to realize it.
Another thing that we hope to do is to make a lot of doctors and health
professionals understand that past medical practice and medical science
are only an accumulation of experience, and do not offer any understanding
of nature at all. We can do this by showing examples of the
possibility of predictable medical practice and individual medical
care using a ten quadrillion speed computer. Moreover, they may
be able to understand that “future life science, medical practice
and medical science will proceed in such a direction.” Even if I say
that “the present time is at the stage of Galileo,” the people in
clinical practice cannot understand this. If we can show concrete
examples, however, I believe that our message, “we have to change
our thinking in the future”, can be delivered.
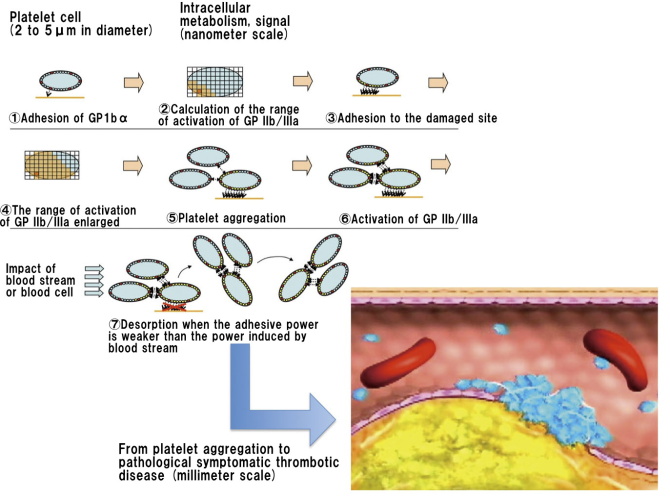
■Research and development of platelet cell simulator
━ What is the platelet cell simulator that you are addressing now?
●Goto Platelet cells are divided by voxels, and the properties
of subcellular organelle and membrane protein are included in
each voxel to reconstitute platelet cells. If the number of divisions
is increased, it can be expected that it can be reduced to a single
cell. As concerns the adhesive protein of a cell membrane, at the
present time, we are aiming at coupling with information about
adhesiveness obtained in a molecular scale structural analysis. Since
treatment with antiplatelet drugs for prevention of recurrence of myocardial
infarction that we provide as clinicians is intervention to molecules such
as cyclo-oxygenase in platelets, platelet membrane protein and receptor
protein, we are aiming at a simulation of how molecular scale intervention
with a drug may change the behavior of platelet cells. Finally, I want to
simulate whether or not organ-perfusing arteries which perfuse important
organs such as the heart and brain may be thrombotically occluded by
aggregation of a large number of platelet cells, and whether or not the
occlusion can be inhibited by intervention with a drug of molecular scale.
As for the molecules constituting platelet cells, moreover, there are
molecules with obvious biological characteristics such as adhesive proteins
having special adhesion modes. I therefore think that the platelet cell
simulator will be useful for combination of the molecular scale with the cell
scale. Since it is known that aggregation of a large number of platelet cells
may cause myocardial infarction, moreover, the simulator will promote a
combination of the cell scale with the organ and body scale. Moreover, this
is a system to prepare the basis of a 2-step coupling of the molecular scale
with the cell scale, and the cell scale with the organ and body scale, mainly
with platelet cells, by coupling the associations between molecules and
platelet cells theoretically by simulation, and by quantitatively simulating
the process in which platelet cells of micrometer scale lead to occlusion of
blood vessels of millimeter scale, that is, the impact of cells on the organs
and body.
A platelet cell has no nucleus and is not divided. Moreover, there is less
production of new substances. Its function is specialized in hemostasis
and thrombus formation. Since platelet cells have a simple structure and
function, it is suitable for reproduction by simulation. I will show an actual
example using platelet cells. Moreover, it is clear from clinical studies that
platelet cells are importantly involved in the onset of myocardial infarction
and cerebral infarction and that, if the function of platelet cells is reduced,
the onset of myocardial infarction and cerebral infarction is inhibited. From
the viewpoint of clinical medicine, the association of the intervention with
a drug on the molecular scale and the outcome of the organ and body scale
are obvious. Finally, whether or not a correct simulation can be performed
from the viewpoint of physics and technology is important. However,
biological cells are very complex, and it is very difficult to perform a precise
simulation. Collection of actual information in the body and modeling it
on a computer should progress like two wheels of a cart. It cannot be said
that the information to be entered into the computer is sufficient, and its
quantitative capability is also low. Platelet cells are relatively easily handled,
but this is a very difficult challenge as a project.
━ What is the most difficult thing in developing a simulator?
●Goto I recognize that the biggest problem is that we have not understood the whole picture. Even if Kei becomes available, it is still impossible to reproduce the complex biological body. A certain simplification is essential. Simplification by us who have not understood the whole picture may be beyond the mark. Since calculation resources are limited, we are selecting the information to be omitted in our brain. You might think that the computer is fully automatic, but it is the human brain that enters important information to make a model. Our worst problem is that we do not know whether or not modeling can be done by selection of appropriate information. Comparing the secret of the human body pursued in medical science to the secret of the universe, I do not know whether, in the vast universe, our current anxiety is because we only know the circumference of the earth, we only know the solar system, we only know up to the galaxy, or we actually know a considerable amount. Even if we only knew up to the solar system, it might still be possible to clarify the basic principle controlling the universe. At the present time, we have to try to predict the phenomena of the human body and the outcome of disease using a principle which we definitely understand. By substantiating the validity of the predicted result, the validity of the prediction will be confirmed. In simulation science on a subject that has not revealed its true aspect, it is essential to repeat prediction and substantiation. It is a challenging academic field from the viewpoint that the validity of modeling is repeatedly being confirmed, while the truth has not yet been observed. I am a clinician and actually provide medical care. I actually feel that much of clinical practice depends on my experience and feeling. Although we cannot find a scientific rationale, moreover, we are practicing individualized medical care based on my experience and feeling. I am always puzzling over how to select the direction in which we should go for logical performance and digitization of individualized medical science, not based on science conducted empirically by a lot of doctors.
━ How about the reaction of medical practice to your approach?
●Goto I think that the meaning of what I want to show can be
understood by everybody. Particularly, the leaders in academic societies
say, “certainly, we have to go in such the direction.” The leaders in global
academic societies commonly recognize that the method called Evidence-
Based Medicine, that is, a scientific approach to medical practice by building
a numerical database by accumulating present experience, has got stuck.
Medical practice and medical education are suffering from a flood of
information to the numerical database of experience. It is difficult to get
healthcare professionals to change their mind and realize that predictive and
individual medical care is required. In order that the validity of our approach
is understood by healthcare professionals, moreover, it is important to show
an actual example of antiplatelet treatment using a platelet cell simulator as
an example. I want a lot of people to understand that even life phenomena
are ultimately an accumulation of physical and chemical phenomena, and
its descriptive term is mathematics. Moreover, I expect that young doctors,
researchers and students will participate in the field of simulation medicine.
I think that the quadrillion speed computer is the gateway to it.
BioSupercomputing Newsletter Vol.4
- SPECIAL INTERVIEW
- In order to change from observation-type medical practice focusing on experience to prediction-type medical practice to construct the base of theoretical medicine
Professor, Department of Internal Medicine (Cardiovascular Medicine), Director of the Metabolic Disease Research Center, Bio-Research Medical Center, Tokai University Graduate School of Medicine, and Director, Department of Metabolic System Medicine, Tokai University General Medical Laboratory Shinya Goto - It is expected that new possibilities in nutrition science and health control will be opened up
by simulation science
EXECUTIVE PROFESSIONAL Health infomatics DEPT., Ajinomoto Co., Inc. Toshihiko Ando
- Report on Research
- The functions of a multidrug discharging transporter were verified by coarse graining molecular simulation (Molecular Scale WG)
Graduate School of Science, Kyoto University Shoji Takada / Xin-Qiu Yao / Hiroo Kenzaki - Cell simulation considering time-space (Cell Scale WG)
Computational Science Research Program, RIKEN Yasuhiro Sunaga - Development of HIFU simulator for non-invasive treatment with high-intensity focused ultrasound (Organ and Body Scale WG)
VCAD System Research Program, RIKEN Kohei Okita - PLATO: Platform for a collaborative brain system modeling toward development of large scale mathematical model.(Brain and Neural WG)
①Computational Science Research Program, RIKEN
②Brain Science Institute, RIKEN
Keiichiro Inagaki①/ Takayuki Kannon②/ Nilton L. Kamiji②/ Koji Makimura②/ Shiro Usui ①②
- Report
- Report on the workshop in BMB2011 (Joint Meeting of the 33rd Congress of the Molecular Biology Society of Japan and the 83th Congress of the Japanese Biochemical Society)
- Winter School 2011 for the Integrated Simulation of Living Matter
Computational Science Research Program, RIKEN Yasuhiro Ishimine (Organ and Body Scale WG)
The Institute of Medical Science, The University of Tokyo Hidetoshi Urakubo (Brain and Neural WG)
Computational Science Research Program, RIKEN Yasuhiro Sunaga (Cell Scale WG)
Computational Science Research Program, RIKEN Gen Masumoto (High-Performance Computing Team)
Computational Science Research Program, RIKEN Keiji Misawa (Data Analysis Fusion WG)
Computational Science Research Program, RIKEN Hisayuki Miyashita (Molecular Scale WG) - Winter School 2011 for the Integrated Simulation of Living Matter